The American Heart Association released its comprehensive 2025 Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care in October 2025, marking the most significant update to resuscitation science in five years. With 760 specific recommendations spanning adult, pediatric, and neonatal life support, these guidelines introduce critical changes that every healthcare provider needs to understand and implement immediately.
At Project Heartbeat, all of our BLS, ACLS, and PALS courses have been updated to reflect these latest 2025 guidelines. Whether you’re due for recertification or want to ensure your team is trained on the most current protocols, our HeartCode Complete courses and traditional classroom training incorporate every change outlined below.
What’s Different About the 2025 Guidelines?
The 2025 guidelines represent a comprehensive review of resuscitation science conducted by the International Liaison Committee on Resuscitation (ILCOR). Interestingly, only 1.4% of the 760 recommendations are based on Level A evidence (high-quality randomized controlled trials), highlighting the ongoing challenges in performing high-quality resuscitation research and the continued need for evidence-based studies in emergency cardiovascular care.
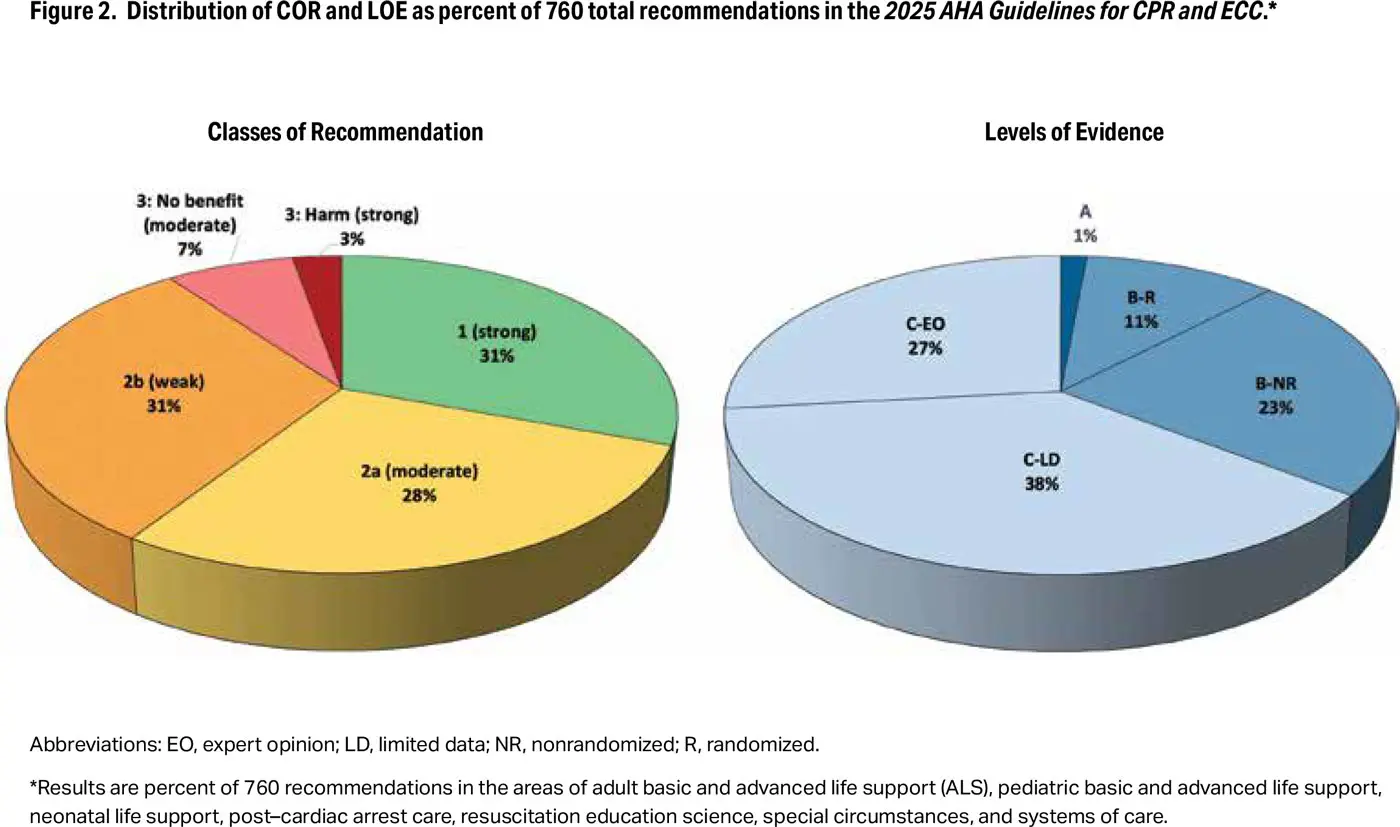
Credit: © 2025 American Heart Association. Source: Highlights of the 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
Despite this, several evidence-based changes have been made that will significantly impact how healthcare providers perform CPR, manage airways, administer medications, and provide post-cardiac arrest care.
 MAJOR BLS (Basic Life Support) CHANGES
MAJOR BLS (Basic Life Support) CHANGES
1. Foreign Body Airway Obstruction Protocol – SIGNIFICANT CHANGE
This is the most visible change for both healthcare providers and the public.
OLD Protocol (2020):
- Adults: Start with abdominal thrusts (Heimlich maneuver)
- Children: Start with abdominal thrusts
- Infants: Alternating back blows and chest thrusts
NEW Protocol (2025):
- Adults: Repeated cycles of 5 back blows followed by 5 abdominal thrusts
- Children: Repeated cycles of 5 back blows followed by 5 abdominal thrusts
- Infants: Repeated cycles of 5 back blows followed by 5 chest thrusts (unchanged)

Credit: © 2025 American Heart Association. Source: Highlights of the 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
Why It Matters: Recent observational studies of adult and pediatric choking incidents demonstrated that back blows (back slaps) were associated with improved clearance rates and fewer injuries compared to abdominal thrusts alone. By starting with back blows for all age groups, the AHA has created consistency across all populations and simplified training for both healthcare providers and lay rescuers.
For pregnant patients or when the rescuer cannot encircle the abdomen, use 5 chest thrusts instead of abdominal thrusts.
Clinical Impact: Emergency departments should expect to see fewer abdominal injuries related to choking interventions as back blows become the first-line approach.
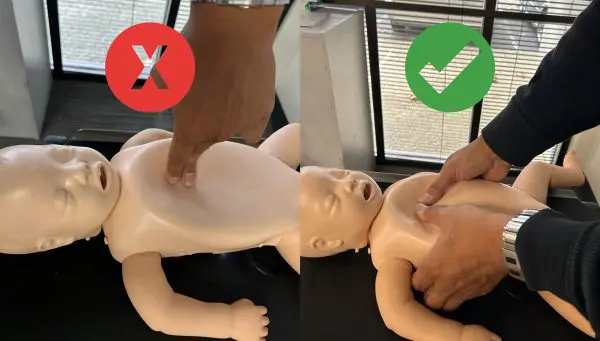
2. Infant CPR Hand Position – Major Technique Change
OLD Recommendations:
- 2-finger technique (primary)
- 2-thumb encircling hands technique (alternative)
- Heel of 1 hand (mentioned for larger infants)
NEW Recommendations (2025):
- Heel of 1 hand OR 2-thumb encircling hands technique (recommended)
- 2-finger technique NO LONGER RECOMMENDED
Why It Matters: A multicenter prospective observational study found that the 2-finger technique consistently failed to achieve adequate compression depth and rarely met AHA guidelines for infant CPR quality metrics. In contrast, both the heel-of-1-hand technique and 2-thumb encircling technique achieved significantly greater compression depth with better consistency.
What This Means for Training: Healthcare providers trained in the 2-finger technique must retrain to use either heel-of-1-hand or 2-thumb encircling hands. The 2-thumb technique remains optimal when multiple rescuers are present, while heel-of-1-hand is recommended when the rescuer cannot physically encircle the infant’s chest.
3. Defibrillation Pad Placement for Women
NEW Recommendation (2025): When placing defibrillation pads, it may be reasonable to adjust the position of a bra instead of removing it.
Why It Matters: Women experience significantly lower rates of public-access defibrillation compared to men. Research suggests that the need to expose a woman’s chest to apply pads may be a contributing barrier. By allowing rescuers to adjust rather than remove a bra, this recommendation aims to reduce hesitation and increase willingness to use AEDs on women in cardiac arrest.
Pads must still be placed directly on bare skin – this recommendation simply provides an alternative to complete bra removal when adjustment allows for proper pad placement.
4. Mechanical CPR Devices – Clear Guidance

OLD: Recommendations were unclear about routine use
NEW (2025):
- The routine use of mechanical CPR devices is NOT recommended for adult cardiac arrest
- May be considered in specific settings where high-quality manual compressions are challenging or dangerous for healthcare professionals, provided interruptions during deployment are minimized
Why It Matters: Numerous randomized controlled trials have demonstrated no survival benefit from mechanical CPR devices compared to high-quality manual compressions. However, the guidelines acknowledge that specific circumstances—such as prolonged transport, cardiac catheterization lab procedures, or ECPR preparation—may warrant mechanical device use when manual CPR quality would be compromised.
5. Ventilation During CPR – Renewed Emphasis
NEW Emphasis (2025):
- Give enough tidal volume to produce visible chest rise
- Avoid both hypoventilation (too few/too little) and hyperventilation (too many/too much)
- When providing rescue breaths for respiratory arrest: 1 ventilation every 6 seconds (10 breaths/min)
Why It Matters: Recent studies identified that rescuers often fail to deliver adequate ventilation during CPR. Research demonstrated that CPR with both effective chest compressions AND effective ventilation was associated with improved outcomes. The emphasis on visible chest rise helps rescuers deliver appropriate tidal volumes.
Compression-to-Ventilation Ratio Reaffirmed: 30:2 remains the standard before placement of an advanced airway, for both lay rescuers and healthcare professionals.
6. CPR for Patients with Obesity
NEW (2025): CPR for adults with obesity should be provided using the same techniques as for patients without obesity.
Why It Matters: A 2024 ILCOR scoping review of 34 observational studies found no evidence to support modifications to standard CPR technique for patients with obesity. This recommendation prevents hesitation and ensures consistent, high-quality CPR for all patients.
7. Trauma and Airway Management
UPDATED (2025): For adults with head and neck trauma, if the airway cannot be opened with a jaw thrust and airway adjunct insertion, trained rescuers should open the airway using a head tilt-chin lift.
Why It Matters: Opening the airway is the priority in trauma patients. While jaw thrust is preferred to minimize cervical spine movement, establishing a patent airway for oxygenation and ventilation takes precedence when jaw thrust is unsuccessful.
MAJOR ACLS (Advanced Cardiovascular Life Support) CHANGES
1. Vascular Access: Clear Hierarchy Established
NEW Clear Recommendation (2025):
- IV access is RECOMMENDED as the first choice for drug administration in cardiac arrest
- IO (intraosseous) access is REASONABLE if initial IV attempts are unsuccessful or not feasible
Why It Matters: A 2025 ILCOR systematic review including three recent large randomized controlled trials found that IO access compared with IV access was associated with lower rates of achieving sustained ROSC. While IO remains a valuable rescue option when IV access cannot be established, the evidence now supports prioritizing IV access when possible.
Clinical Impact: EMS systems and hospital code teams should emphasize IV access skills and consider IO as backup rather than equal first choice.
2. Epinephrine Timing for Shockable Rhythms
UPDATED Recommendation (2025): For patients in cardiac arrest with a shockable rhythm, it is reasonable to administer epinephrine AFTER initial defibrillation attempts have failed.
Why It Matters: The evidence supports prioritizing rapid defibrillation over medication administration for shockable rhythms. Epinephrine should be administered after CPR and defibrillation are unsuccessful, not as a first-line intervention alongside initial shocks.
Timeline: This typically means giving epinephrine after 2-3 failed defibrillation attempts while continuing high-quality CPR.
3. Vasopressin – Issue Settled
 UPDATED (2025): Vasopressin alone or vasopressin in combination with epinephrine offers NO advantage as a substitute for epinephrine in cardiac arrest.
UPDATED (2025): Vasopressin alone or vasopressin in combination with epinephrine offers NO advantage as a substitute for epinephrine in cardiac arrest.
Why It Matters: Multiple systematic reviews and meta-analyses have consistently found no difference in survival outcomes when comparing vasopressin (alone or combined) versus epinephrine alone. This settles a long-standing question in resuscitation medicine.
Clinical Impact: Stop stocking and using vasopressin for cardiac arrest – epinephrine is the sole recommended vasopressor.
4. Alternative Defibrillation Strategies – Insufficient Evidence
NEW (2025):
- Vector Change Defibrillation: Usefulness “not well established” for refractory VF/pVT
- Double Sequential Defibrillation: Usefulness “not well established” for refractory VF/pVT
Why It Matters: Despite industry interest and theoretical benefits, current evidence from clinical trials is insufficient to recommend either vector change or double sequential defibrillation as routine strategies. A single small RCT supports their use, but numerous questions remain about timing, pad placement, and patient selection.
Clinical Guidance: Continue standard defibrillation protocols; these alternative strategies remain investigational.
5. Cardioversion Energy Levels – Higher is Better
UPDATED (2025):
- Atrial Fibrillation: Initial energy setting of ≥200J is reasonable (increased from previous recommendations)
- Atrial Flutter: 200J may be reasonable for initial cardioversion
Why It Matters: Recent randomized trials involving over 3,000 patients with atrial fibrillation found that 200J shocks achieved >90% cumulative cardioversion success across all three currently available US biphasic defibrillator platforms. Lower energy settings were associated with higher failure rates and the need for repeat shocks.
Additionally, low-energy monophasic shocks were more likely to provoke ventricular fibrillation when cardioverting AF compared to higher energy (≥200J) biphasic shocks.
Clinical Impact: Start with 200J for AF/flutter cardioversion rather than traditional lower energy levels.
6. Head-Up CPR – Not Recommended
NEW (2025): Head-up CPR is NOT recommended except in the setting of clinical trials.
Why It Matters: A recent ILCOR systematic review found no RCTs and only 3 observational studies with significant methodological limitations. The evidence certainty is “very low” for any benefit on survival or favorable neurologic outcome.
Clinical Guidance: Despite device availability and marketing, head-up CPR should not be implemented outside research protocols.
7. Other Antiarrhythmic Medications
NEW (2025): For adults in cardiac arrest, the use of β-blockers, bretylium, procainamide, or sotalol for VF/pVT unresponsive to defibrillation is of uncertain benefit.
Why It Matters: No new evidence supports these alternative antiarrhythmic agents. Amiodarone and lidocaine remain the recommended antiarrhythmic options during cardiac arrest.
Note: Bretylium tosylate was recently reintroduced to the US market, but no new evidence supports its effectiveness or safety compared to current recommendations.
8. Post-Cardiac Arrest: Blood Pressure Targets
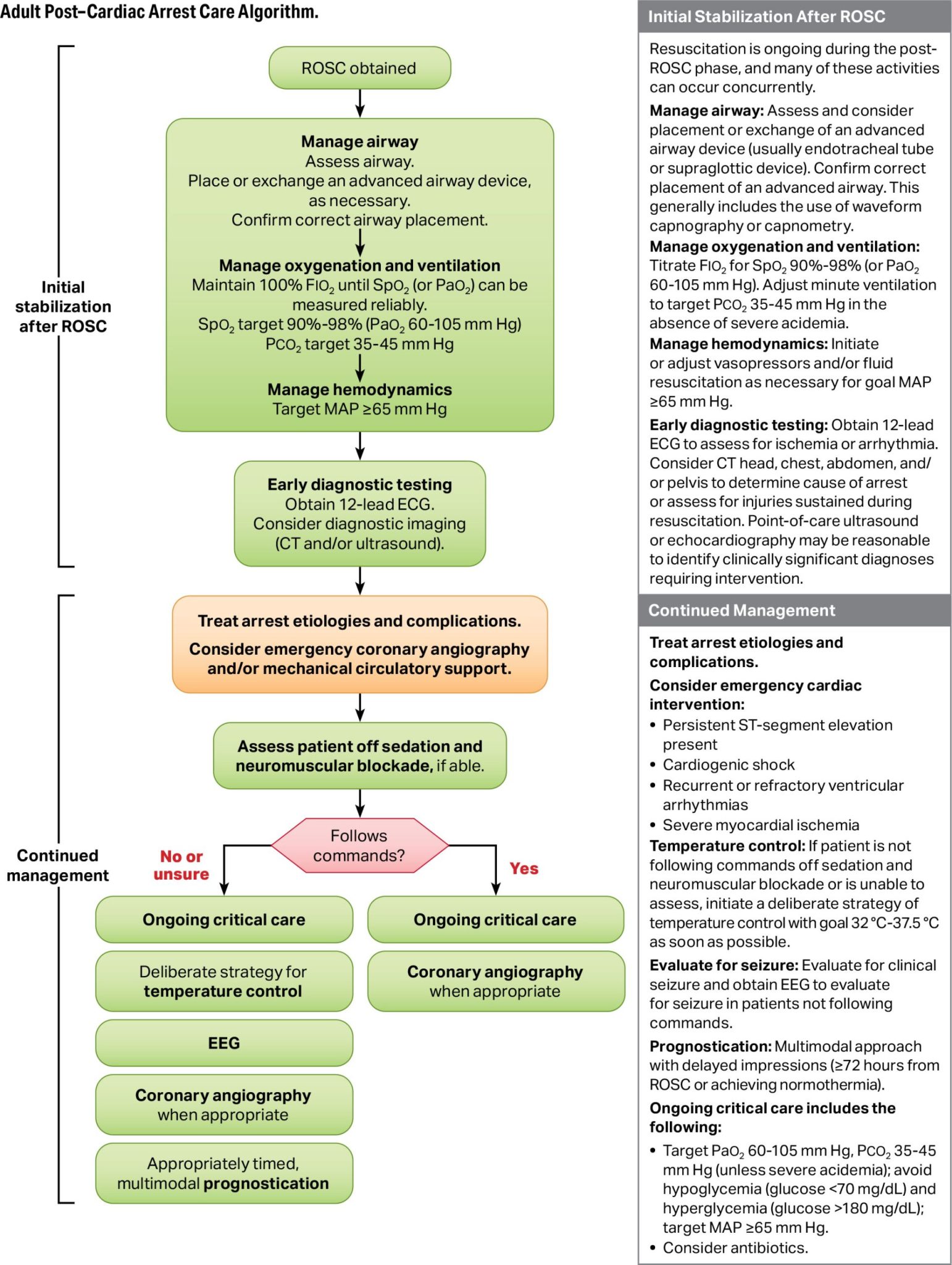
Credit: © 2025 American Heart Association. Source: Highlights of the 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
UPDATED (2025): Hypotension should be avoided after ROSC by maintaining a minimum MAP of at least 65 mmHg.
Why It Matters: Four randomized trials compared lower versus higher MAP targets after OHCA and found no benefit from targeting higher MAP (e.g., 80-100 mmHg). A minimum MAP of 65 mmHg represents appropriate balance between avoiding hypotension and preventing potential harms of excessive vasopressor use.
MAJOR PALS (Pediatric Advanced Life Support) CHANGES
1. Epinephrine Timing – Early is Critical
UPDATED (2025): For infants and children in cardiac arrest with initial non-shockable rhythm, it is reasonable to administer the first dose of epinephrine as early as possible.
Why It Matters: A systematic review of 7 observational studies identified that shorter time to first epinephrine dose was associated with increased rates of favorable outcome in both OHCA and IHCA. Time to first dose <3 minutes was associated with the highest rates of favorable outcome, though there was no direct comparison across different time intervals.
Clinical Impact: Pediatric resuscitation teams should prioritize rapid vascular access and early epinephrine administration for non-shockable rhythms rather than prolonged attempts at establishing perfect IV access.
2. Hemodynamic Monitoring During CPR
NEW (2025): For infants and children with continuous invasive arterial blood pressure monitoring during CPR, it may be reasonable to target specific diastolic blood pressures:
- Infants: Diastolic BP ≥25 mmHg
- Children ≥1 year: Diastolic BP ≥30 mmHg
Why It Matters: A new multicenter study demonstrated that among pediatric patients with an arterial line during CPR, achieving these diastolic BP thresholds was associated with improved survival with favorable neurologic outcome.
Clinical Application: When arterial line monitoring is available during pediatric resuscitation, use real-time diastolic BP feedback to optimize CPR quality and hemodynamic support.
3. ETCO2 Monitoring – Use with Caution

UPDATED (2025): For infants and children with invasive airways during CPR, ETCO2 monitoring may be considered to monitor CPR quality.
CRITICAL NEW GUIDANCE: A specific ETCO2 cutoff value alone should NOT be used as an indication to end resuscitative efforts in infants and children.
Why It Matters: While ETCO2 values ≥20 mmHg during CPR were associated with increased odds of ROSC and survival in a recent multicenter study, survival has been documented in patients with average ETCO2 <20 mmHg. Using a single cutoff value could lead to premature termination of potentially viable resuscitations.
Clinical Guidance: Use ETCO2 as one of multiple factors when considering termination of resuscitation, never as the sole criterion.
4. Post-Arrest Blood Pressure Management
UPDATED (2025): After cardiac arrest in infants and children, it is recommended to maintain systolic and mean arterial blood pressure >10th percentile for age.
Why It Matters: Post-arrest hypotension (blood pressure <5th percentile for age) occurs in 25-50% of pediatric cardiac arrest survivors and is associated with decreased rates of survival to discharge. A secondary analysis of the ICU-Resuscitation trial found higher survival rates when blood pressure targets exceeded the 10th percentile during the first 6 hours post-arrest.
Specific Targets:
- Systolic BP >10th percentile for age
- Diastolic BP >50th percentile for age
5. Neuroprognostication – Multimodal Approach Required
NEW (2025): It is recommended that healthcare professionals consider multiple modalities when predicting neurological outcomes (favorable or unfavorable) after resuscitation from cardiac arrest in infants and children.
Key Points:
- No single test is reliable in isolation for predicting outcome
- EEG is reasonable up to 72 hours post-arrest when interpreted with other prognostic criteria
- Cough/gag reflexes and pain response are NOT well established for prognosis
- Multiple systematic reviews evaluated neurological examination, biomarkers, EEG, and neuroimaging – none met prespecified accuracy for use as lone prognostic criterion
Clinical Impact: Avoid premature withdrawal of life-sustaining therapies based on a single test result. Use comprehensive, multimodal assessment over time.
6. Post-Arrest Recovery and Survivorship

UPDATED (2025): It is reasonable that infants and children who survive cardiac arrest be evaluated for physical, cognitive, and emotional needs to guide follow-up care within the first year following cardiac arrest.
Why It Matters: Recovery from cardiac arrest extends long after initial hospitalization. Survivors may require ongoing integrated medical, rehabilitative, caregiver, and community support in the months to years after cardiac arrest. A recent AHA scientific statement highlights the importance of supporting patients and families to achieve the best possible long-term outcome.
Recommended Assessments:
- Physical function and rehabilitation needs
- Cognitive function and educational support
- Emotional/psychological health
- Family/caregiver support needs
SPECIAL CIRCUMSTANCES UPDATES
1. Opioid Overdose – Naloxone Recommendations
NEW (2025): For lay and trained rescuers, opioid antagonist administration (eg, naloxone) may be reasonable for adults and children in cardiac arrest with suspected opioid overdose, provided that naloxone administration does not interfere with delivery of standard resuscitation, including high-quality CPR with breaths.
NEW (2025): Adults and children treated for opioid overdose should receive an opioid antagonist (eg, naloxone) and instruction on how to use it at the time of discharge from a healthcare setting.
Why It Matters: Opioid antagonists restore protective airway reflexes and reverse respiratory arrest. While no clinical trials have evaluated naloxone in cardiac arrest, there is no known harm from administration if it doesn’t delay CPR. “Take-home” naloxone programs can prevent future fatal overdoses.
2. Cardiac Arrest During Pregnancy
UPDATED (2025): Preparation for resuscitative delivery (replacing the term “perimortem cesarean delivery”) should begin at recognition of cardiac arrest, with the goal to complete delivery by 5 minutes.
NEW (2025): It is reasonable to use ECPR in pregnant or peripartum patients in cardiac arrest not responsive to standard resuscitation.
NEW (2025): A massive transfusion protocol with balanced transfusion strategy should be used for peripartum patients with suspected life-threatening amniotic fluid embolism.
Why It Matters: Studies for ECPR in pregnant patients reported survival rates between 55-75%. Resuscitative delivery within 5 minutes improves outcomes for both the pregnant patient and fetus. Amniotic fluid embolism is characterized by hemorrhage and DIC – balanced massive transfusion reduces mortality.
3. Left Ventricular Assist Devices (LVADs)
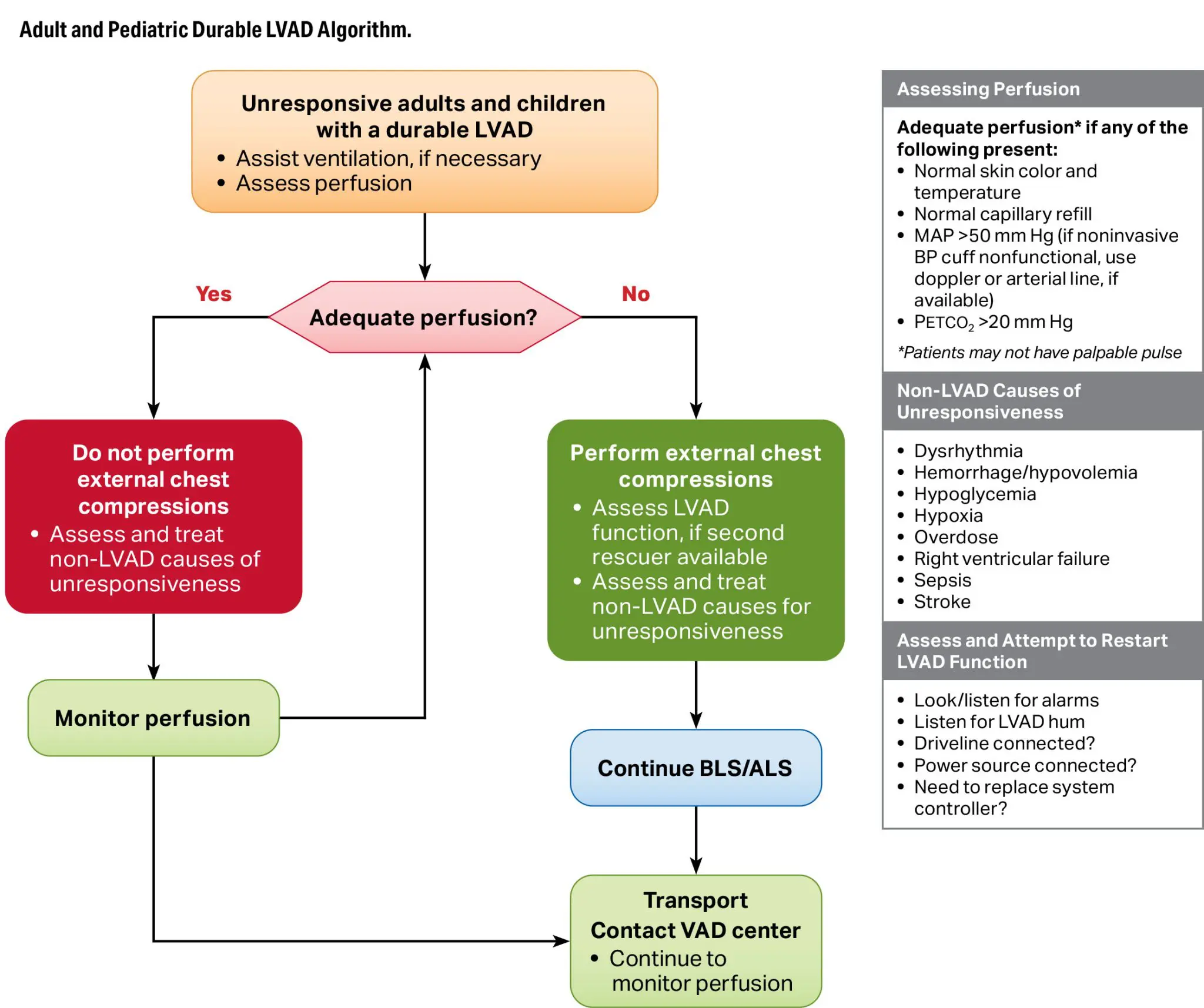
© 2025 American Heart Association. Source: Highlights of the 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
NEW (2025): In unresponsive adults and children with durable LVADs and impaired perfusion, chest compressions should be performed.
NEW (2025): It may be reasonable to start chest compressions immediately while simultaneously assessing for device-related reversible causes.
Why It Matters: The absence of a palpable pulse makes confirming cardiac arrest difficult in LVAD patients. Impaired perfusion (assessed by skin color/temperature, capillary refill, MAP, ETCO2) indicates likely cardiac arrest. The potential benefit of CPR outweighs the theoretical risk of device dislodgment.
4. Life-Threatening Hypothermia
NEW (2025): It is reasonable to use prognostication scores (HOPE probability score, ICE survival score) to guide the decision for initiating ECLS rewarming for adults and children in hypothermic cardiac arrest.
NEW (2025): It may be reasonable to rewarm adults and children with severe environmental hypothermia (core temperature <28°C [84°F]) and NOT in cardiac arrest using ECLS.
Why It Matters: Severe hypothermia can cause cardiac arrest and findings that mimic death, but reduced metabolic rate increases likelihood of neurologically intact survival. Studies show improved survival with ECLS compared to conventional CPR for hypothermic cardiac arrest.
EDUCATION & TRAINING UPDATES
Feedback Devices – Now Recommended
UPDATED (2025): Feedback devices are RECOMMENDED for use during CPR training for both healthcare professionals and lay rescuers.
Why It Matters: Meta-analysis of RCTs demonstrated that CPR feedback devices had a moderate to large effect on all CPR quality metrics for both healthcare professionals and lay rescuers.
Virtual Reality – Mixed Recommendations
NEW (2025):
- VR may be reasonable to support knowledge acquisition in BLS and ACLS training
- VR should NOT be used to teach CPR skills
Why It Matters: New data shows VR is useful for cognitive learning but inferior for skills training. Studies found VR-based CPR skills training was either inferior to or no different from traditional training for quantitative skill parameters (depth, rate).
Disparities in CPR Education – Action Required
UPDATED (2025): It is RECOMMENDED to:
- Focus and tailor lay rescuer CPR training to specific racial and ethnic populations
- Address barriers to performing CPR on women through educational training
- Focus on low socioeconomic status populations and neighborhoods
- Address barriers to linguistically isolated communities
Why It Matters: Known disparities exist in both patients who receive CPR and availability of CPR training. Focusing on specific populations and modifying education to address differences could eliminate disparities and enhance cardiac arrest outcomes.
WHAT THESE CHANGES MEAN FOR YOU
For Healthcare Providers:
✓ Recertification is Required: If you hold BLS, ACLS, or PALS certification from before October 2025, you’ll need to recertify to learn the new protocols.
✓ Your Current Certification Remains Valid: Existing certifications remain valid until their expiration date, but you should familiarize yourself with key changes immediately.
✓ Practice Changes: Several changes (FBAO protocol, infant CPR technique, medication timing) require immediate implementation in clinical practice.
✓ Team Training: Code teams should review new algorithms together, especially changes to FBAO, vascular access priorities, and hemodynamic targets.
For Training Centers:
✓ Course Materials Must Be Updated: All BLS, ACLS, and PALS training materials should reflect 2025 guidelines.
✓ Instructor Training: Instructors need retraining on new techniques, especially FBAO and infant CPR hand positions.
✓ Manikin Skills Stations: Update skills stations to teach back blows first for choking and eliminate 2-finger infant CPR demonstrations.
For EMS Systems & Hospitals:
✓ Protocol Updates: Medical directors should update system protocols to reflect 2025 guidelines, particularly regarding:
- Vascular access preferences (IV first)
- Epinephrine timing for shockable rhythms
- Blood pressure targets post-arrest
- FBAO management
✓ Equipment Changes: Consider removing vasopressin from code carts; ensure adequate naloxone availability.
✓ Quality Improvement: Use new hemodynamic targets for CPR quality feedback when available.
GET TRAINED ON THE 2025 GUIDELINES
At Project Heartbeat, we’ve already updated all of our courses to reflect the 2025 AHA Guidelines. Whether you’re getting certified for the first time or renewing your credentials, you can be confident you’re learning the most current, evidence-based resuscitation protocols.
Our 2025 Guidelines-Based Courses:
HeartCode Complete BLS, ACLS & PALS
- Self-paced online learning + hands-on skills verification
- Reflects all 2025 guideline changes
- Complete on your schedule
- Available at 40 locations across 5 states
Traditional Classroom Courses
- Expert instructor-led training
- Comprehensive hands-on practice
- Small class sizes
- Oakland and Sacramento campuses
Find Your Nearest Location: With 40 HeartCode CPR Verification Stations across California, Arizona, Colorado, Nevada, Oregon, and Washington, there’s a Project Heartbeat location near you.
DOWNLOAD THE OFFICIAL GUIDELINES
Want to dive deeper into the 2025 Guidelines? Access the official AHA publications:
📄 2025 Guidelines Highlights (Free PDF)
📄 Full Guidelines (Circulation, October 2025)
📄 ILCOR Consensus on Science (Free Access)
FREQUENTLY ASKED QUESTIONS
Q: When do I need to recertify if I was certified under the 2020 guidelines?
A: Your current certification remains valid until its expiration date (typically 2 years from issue). However, we recommend familiarizing yourself with the key changes immediately and implementing them in clinical practice. When it’s time to recertify, choose a course that reflects the 2025 guidelines.
Q: What’s the most important change I need to know right now?
A: The FBAO (choking) protocol change is the most immediately visible – you should start using 5 back blows before abdominal thrusts for adults and children. For infant CPR, eliminate the 2-finger technique and use heel-of-1-hand or 2-thumb encircling instead.
Q: Are the algorithms significantly different?
A: Most algorithms have minor updates rather than major overhauls. The Adult FBAO Algorithm is new, and the Post-Cardiac Arrest Care Algorithm has updates. The basic BLS and ACLS algorithms remain structurally similar with refinements in timing and techniques.
Q: Will my AHA certification card indicate which guideline version I trained under?
A: AHA certification cards don’t typically specify guideline year, but your training date indicates which guidelines were current. Courses completed after October 2025 should reflect the 2025 guidelines.
Q: Do I need to update my hospital’s code blue protocols?
A: Yes, medical directors should review and update protocols to reflect 2025 guidelines, particularly regarding vascular access preferences, medication timing, hemodynamic targets, and FBAO management. Work with your pharmacy to remove vasopressin from code carts.
Q: Where can I get trained on the new infant CPR technique?
A: All of Project Heartbeat’s BLS and PALS courses now include training on the updated infant CPR hand positions. You can take HeartCode Complete courses at any of our 40 locations or attend traditional classroom training at our Oakland or Sacramento campuses.
STAY CURRENT WITH PROJECT HEARTBEAT
[NEWSLETTER SIGNUP SECTION]
Don’t miss important updates about resuscitation guidelines, certification requirements, and training best practices.
📧 Subscribe to our quarterly newsletter for:
- Guideline updates and clarifications
- Training tips and best practices
- New location announcements
- Special offers for certification courses
CONCLUSION
The 2025 AHA Guidelines represent the culmination of years of resuscitation research and clinical evidence review. While most changes are refinements rather than revolutionary shifts, several key updates—particularly the FBAO protocol change and infant CPR technique modification—require immediate attention and retraining.
At Project Heartbeat, we’re committed to providing the highest quality, most current training in resuscitation science. All of our courses reflect these latest guidelines, ensuring you receive evidence-based education that prepares you to save lives.
Ready to update your skills? Find a course near you today.